

Fistic Medicine: Examining a Knee Injury
Matt Pitt Jun 2, 2010

Dave Mandel/Sherdog.com
The human knee is beautifully designed for the majority of what man has asked of it in the last 500,000 years. The simple structure is near ideal for following the perambulations of migrating antelope or fleeing predation from the alpha predators primitive man evolved among. However, as Jared Hess demonstrated in his bout with Alexander Shlemenko last Thursday at Bellator 20, the dynamics of an MMA fight can far exceed what nature designed the knee to endure.
Advertisement
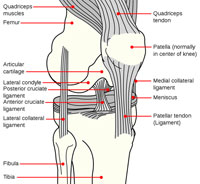
To either side of the joint, providing stability against forces applied to the sides of the knee, are the medial and lateral collateral ligaments. It was one of these, the LCL, that Hess felt give way in the first takedown of the first round, well before anyone but the fighter and the referee noticed anything amiss.
“It popped,” said Hess, who fought on an injured left knee for more
than 10 minutes. “My knee was done. It wasn’t hurting. I just had
no support. I couldn’t push off on it.”
His corner gave him pragmatic advice: take the fight to the ground and keep it there. That worked for the better part of two dominant rounds, until early in the third when Shlemenko got to his feet and got separation.
Public Domain.
Click to Enlarge.
It is probable that this is the exact moment the already injured ligament completely tore. The fact that Hess was able to continue to fight for an additional 77 seconds is remarkable, but not inconceivable; with three of its four ligaments intact, the knee maintains basic anatomic stability. However, as Hess continued to fight, the remaining ligaments -- possibly also injured in the collapse -- were enduring forces for which they were not designed.
When the fight was finally stopped, the first thing the doctor did was bend the knee and pull the tibia forward -- an Anterior Drawer test, checking the competence of the ACL. The leg moved more than it should. The fight was over. Potentially a career as well.
After being evaluated by ER doctors, Hess learned that in addition to a ruptured LCL -- which he had known was shot -- he had a meniscus tear and ligamentous laxity. It could have been worse: Although knee dislocations are rare with isolated LCL tears -- particularly low energy dislocations -- they do occur. If the tibia is disarticulated and driven back into the popliteal artery, severe vascular compromise and even loss of the limb can occur. If the tibia moves laterally and tears the nerves that cross the joint, incapacitating foot drop can occur. Hess’ work-up showed no sign of such injuries.
Currently Hess is waiting to meet with his regular orthopedic surgeon to plan a course of treatment. In this respect he is the beneficiary of the long, broad road paved by football players and their doctors. When a runner is low-tackled from the side, the disruptive forces blow apart the medical collateral ligament (MCL), and often the ACL and meniscus: the "unhappy triad."
The technology developed to repair these injuries is directly applicable to Hess’ damaged knee. Surgery, ideally arthroscopic, is needed for total disruption of the ligament. In the simplest case, the damaged ligament can be sutured back together, or sewn or stapled back into place on the bone from whence it was torn. In more severe cases, the entire ligament needs to be replaced, either with an autograft, perhaps using a portion of Hess’ own hamstring tendon, or a cadaver allograft. Recovery is long but has a high likelihood of being virtually complete.
For many of us, watching and re-watching Hess’ injury, the most amazing aspect of the entire event is not the failing of the athlete’s knee but the success of the warrior’s mind. Fighting and winning the better part of three rounds on an injured knee, succumbing only when simply walking becomes impossible, is a feat as impressive as any knockout of the night. It demonstrates -- beyond strength of bone and muscle -- what truly separates elite athletes from all others.
More Fistic Medicine »
• Fistic Medicine: The Importance of Mouthguards
• The Benefit & Cost of Steroids
• The Biophysics of Taking a Punch
• Dementia Pugilistica & MMA
• Brock Lesnar’s Illness & Recovery
• Becoming Superhuman
• Thiago Alves & ‘Brain Irregularity’
Related Articles




